What Causes Hammertoe Pain
 Overview
Overview
Hammer toe is defined as a deformity in the toe where part of the toe is permanently bent downward resembling a hammer. Two related conditions are mallet toe and claw toe which effect different toe joints in slightly different ways. The key difference is that Hammer toes tends to effect the middle joint in the toe (note: not the middle toe, the middle toe joint). The disease is usually associated with the second largest toe but can effect the third or fourth toe as well. Mallet toe effects the uppermost toe joint whereas claw toe is caused by the tow being held in a cramped ?claw-like? position.
Causes
Footwear can contribute significantly to the development of hammertoes. Shoes that are too small force your toes into a curled position. Over time, your toe tendons adjust to this positioning, causing your toe or toes to hold a hammered shape. Athletes may be especially susceptible, because of the increased forces on the toes from shoes that are too small or tight. Heel elevation in footwear is also problematic, as it causes your toes to be pushed into the shoe?s toe box. Heel elevation additionally contributes to muscle imbalance. A common example of this is when your Achilles tendon-the tendon at the back of your leg that attaches your calf muscles to your heel bone-is too tight, causing the tendons on the top of your foot that attach to your toes to work too hard and hold your toes in an unnatural, elevated position.
 Symptoms
Symptoms
If you have any of these symptoms, do not assume it is due to hammer toe. Talk to your doctor about symptoms such as a toe that curls down, corns on the top of a toe, calluses on the sole of the foot or bottom of the toe, pain in the middle joint of a toe, discomfort on the top of a toe, difficulty finding any shoes that fit comfortably, cramping in a toe, and sometimes Hammer toes also the foot and leg, difficult or painful motion of a toe joint, pain in the ball of the foot or at the base of a toe.
Diagnosis
Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection.
Non Surgical Treatment
If the toes are still mobile enough that they are able to stretch out and lay flat, the doctor will likely suggest a change of footwear. In addition, she may choose to treat the pain that may result from the condition. The doctor may prescribe pads to ease the pain of any corns and calluses, and medications ranging from ibuprofen to steroid injections for the inflammation and pain. Other options for non-surgical treatments include orthotic devices to help with the tendon and muscle imbalance or splinting to help realign the toe. Splinting devices come in a variety of shapes and sizes but the purpose of each is the same: to stretch the muscles and tendon and flatten the joint to remove the pain and pressure that comes from corns.
Surgical Treatment
Ordinary hammertoe procedures often use exposed wires which extend outside the end of toes for 4-6 weeks. Common problems associated with wires include infection where the wires come out of the toe, breakage, pain from hitting the wire, and lack of rotational stability causing the toe to look crooked. In addition, wires require a second in-office procedure to remove them, which can cause a lot of anxiety for many patients. Once inserted, implants remain within the bone, correcting the pain and deformity of hammertoes while eliminating many of the complications specific traditional treatments.
 Prevention
Prevention
As long as hammertoe causes no pain or any change in your walking or running gait, it isn?t harmful and doesn't require treatment. The key to prevention is to wear shoes that fit you properly and provide plenty of room for your toes.
All You Need To Know Regarding Bunions
Overview
 A Bunion is one of the most common foot ailments which usually occur near the joint at the base of the big toe. It is actually a bony protrusion which consists of excess or misaligned bone in the joint. Although they may develop on the fifth or little toe, bunions usually occur at the base of the big toe. In addition to causing pain, a bunion changes the shape of your foot, making it harder to find shoes that fit. The good news however, is that you don?t have to hobble for the rest of your life, bunions can be treated.
A Bunion is one of the most common foot ailments which usually occur near the joint at the base of the big toe. It is actually a bony protrusion which consists of excess or misaligned bone in the joint. Although they may develop on the fifth or little toe, bunions usually occur at the base of the big toe. In addition to causing pain, a bunion changes the shape of your foot, making it harder to find shoes that fit. The good news however, is that you don?t have to hobble for the rest of your life, bunions can be treated.
Causes
You are usually born with a foot type that leads to bunion formation. Flat feet with increased flexibility are most likely to form bunions. Abnormal mechanics increase the bunion formation over time. Other causes of bunions include osteoarthritis, gout, rheumatoid arthritis, trauma, and neurovascular disease.
Symptoms
Bunions starts as the big toe begins to deviate, developing a firm bump on the inside edge of the foot, at the base of the big toe. Initially, at this stage the bunion may not be painful. Later as the toes deviate more the bunion can become painful, there may be redness, some swelling, or pain at or near the joint. The pain is most commonly due to two things, it can be from the pressure of the footwear on the bunion or it can be due to an arthritis like pain from the pressure inside the joint. The motion of the joint may be restricted or painful. A hammer toe of the second toe is common with bunions. Corns and calluses can develop on the bunion, the big toe and the second toe due to the alterations in pressure from the footwear. The pressure from the great toe on the other toes can also cause corns to develop on the outside of the little toe or between the toes. The change in pressure on the toe may predispose to an ingrown nail.
Diagnosis
Orthopaedic surgeons diagnose bunions on the basis of physical examination and weight bearing x-rays. Two angles are assessed, the intermetatarsal angle, that is between the first and second metatarsals (the bones that lead up to the base of the toes). If this angle exceeds 9? (the angle found in the healthy foot) it is abnormal and referred to as metatarsus primus varus. the hallux valgus angle, that is, the angle of the big toe as it drifts toward the small toe. An angle that exceeds 15? is considered to be a sign of pathology.
Non Surgical Treatment
Bunions may be treated conservatively with changes in shoe gear, different orthotics (accommodative padding and shielding), rest, ice and medications. These sorts of treatments address symptoms more than they correct the actual deformity. Surgery, by an orthopedic surgeon or a podiatric surgeon, may be necessary if discomfort is severe enough or when correction of the deformity is desired. Orthotics are splints or regulators while conservative measures include various footwear like gelled toe spacers, bunion toes separators, bunion regulators, bunion splints and bunion cushions. There are a variety of available orthotics (or orthoses) including over-the-counter or off-the-shelf commercial products and as necessary, custom-molded orthotics that are generally prescribed medical devices.
Surgical Treatment
The main goal of surgery is to realign the big toe joint in order to relieve symptoms, correct deformity and restore function. Surgery to remove a bunion is known as a bunionectomy. There are many variations of this operation and the type of surgery performed will vary depending on factors such as the degree of deformity, the strength of the bones, the person's age and the surgeon?s preferred approach. Most surgery involves the removal of the bony outgrowth (exostosis) and the realignment of the bones of the joint. Soft tissue structures such as the ligaments and tendons may be repositioned and the bursa may be removed. The insertion of screws and pins may be required to stabilise the bones in their new, realigned position.
Over-Pronation
Overview
When the ankles over-pronate, it throws everything out of alignment. The bones in the feet can actually shift over time, and the muscles and tendons in the leg and ankle will twist. This places repetitive stress on the ligaments, tendons, joints and muscles of the foot, which can cause injury. If your feet are over-pronating, you may notice your muscles feet unusually tired when you way or stand, or they may ache. But symptoms will vary by your weight, age and activity.
Causes
For those not familiar with the term pronation, you might be familiar with terms related to shoes and pronation such as ?motion control?, ?stability,? and ?neutral cushioned.? The terms motion control and stability are typically associated with the word ?over-pronation? or a foot that is supposedly pronating too much and needs correction. According to the running shoe industry, ?over-pronation? is a biomechanical affliction evident when the foot and or ankle rolls inward past the vertical line created by your leg when standing.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
Look at your soles of your footwear: Your sneaker/shoes will display heavy wear marks on the outside portion of the heel and the inside portion above the arch up to the top of the big toe on the sole. The "wet-foot" test is another assessment. Dip the bottom of your foot in water and step on to a piece of paper (brown paper bag works well). Look at the shape of your foot. If you have a lot of trouble creating an arch, you likely overpronate. An evaluation from a professional could verify your foot type.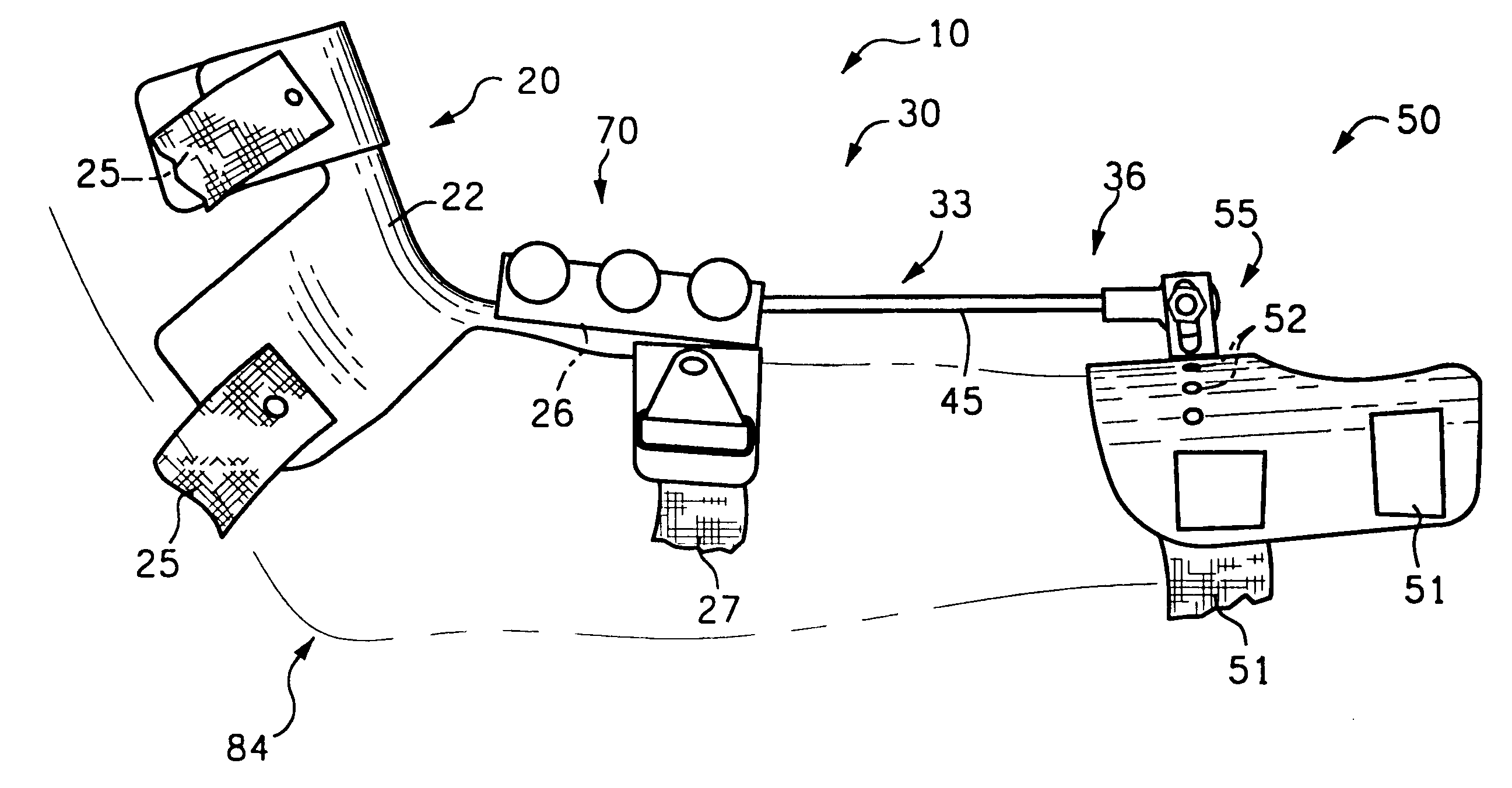
Non Surgical Treatment
If pronation is diagnosed before the age of five it can usually be treated in such a manner that the bones and joints will be aligned properly as growth continues. This may prevent the arch from collapsing, as well as allowing the muscles of the leg to enter the foot without twisting. With proper and early treatment, the foot will not turn out at the ankle, and the child?s gait will improve. Treatment for pronation in children may include: night braces, custom-made orthotics, and exercises. These treatments usually continue until growth is complete, and then the adult may need to wear custom-made orthotics to prevent the pronation from returning (the foot, as every other part of our body, tends to return to its original form if preventive measures are not taken). One side note: frequently, pediatricians will wait too long, hoping that the child will ?outgrow? the problem. By the time they realize that the child?s feet will not improve, it is too late to change the foot. In these cases, custom-made orthotics is used to prevent the pronation from becoming worse.
Prevention
Wearing the proper footwear plays a key role as a natural way to help pronation. Pronated feet need shoes that fit well, provide stability, contain supportive cushioning, are comfortable and allow enough room for your foot to move without causing pain or discomfort. Putting special inner heel wedges, known as orthotics, into your shoes can support a flatfoot while lowering risks of developing tendinitis, according to the American Academy of Orthopaedic Surgeons. More extensive cases may require specially fitted orthopaedic shoes that support the arches.
When the ankles over-pronate, it throws everything out of alignment. The bones in the feet can actually shift over time, and the muscles and tendons in the leg and ankle will twist. This places repetitive stress on the ligaments, tendons, joints and muscles of the foot, which can cause injury. If your feet are over-pronating, you may notice your muscles feet unusually tired when you way or stand, or they may ache. But symptoms will vary by your weight, age and activity.
Causes
For those not familiar with the term pronation, you might be familiar with terms related to shoes and pronation such as ?motion control?, ?stability,? and ?neutral cushioned.? The terms motion control and stability are typically associated with the word ?over-pronation? or a foot that is supposedly pronating too much and needs correction. According to the running shoe industry, ?over-pronation? is a biomechanical affliction evident when the foot and or ankle rolls inward past the vertical line created by your leg when standing.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
Look at your soles of your footwear: Your sneaker/shoes will display heavy wear marks on the outside portion of the heel and the inside portion above the arch up to the top of the big toe on the sole. The "wet-foot" test is another assessment. Dip the bottom of your foot in water and step on to a piece of paper (brown paper bag works well). Look at the shape of your foot. If you have a lot of trouble creating an arch, you likely overpronate. An evaluation from a professional could verify your foot type.
Non Surgical Treatment
If pronation is diagnosed before the age of five it can usually be treated in such a manner that the bones and joints will be aligned properly as growth continues. This may prevent the arch from collapsing, as well as allowing the muscles of the leg to enter the foot without twisting. With proper and early treatment, the foot will not turn out at the ankle, and the child?s gait will improve. Treatment for pronation in children may include: night braces, custom-made orthotics, and exercises. These treatments usually continue until growth is complete, and then the adult may need to wear custom-made orthotics to prevent the pronation from returning (the foot, as every other part of our body, tends to return to its original form if preventive measures are not taken). One side note: frequently, pediatricians will wait too long, hoping that the child will ?outgrow? the problem. By the time they realize that the child?s feet will not improve, it is too late to change the foot. In these cases, custom-made orthotics is used to prevent the pronation from becoming worse.
Prevention
Wearing the proper footwear plays a key role as a natural way to help pronation. Pronated feet need shoes that fit well, provide stability, contain supportive cushioning, are comfortable and allow enough room for your foot to move without causing pain or discomfort. Putting special inner heel wedges, known as orthotics, into your shoes can support a flatfoot while lowering risks of developing tendinitis, according to the American Academy of Orthopaedic Surgeons. More extensive cases may require specially fitted orthopaedic shoes that support the arches.
Physiotherapy And Calcaneal Apophysitis
Overview
Sever's disease involves a lesion to the heel that appears mostly as a result of excessively twisting the ankle. The injury is particularly prevalent in children over 10 and other younger athletes because the heel bone, muscles and tendons are still developing - the bone faster than the muscles - and the condition strikes a growing part of the bone called the calcaneal apophysis. In older people an injury of this sort generally results in a stress fracture.
Causes
There are several theories as to the cause of this condition. These range from a tight Achilles tendon, to micro stress fractures of the calcaneal apopyhsis. The prevailing theory suggests that the condition occurs when the child's growth plate is at its weakest. Combined with increased athletic activity, improper shoe gear and trauma the heel becomes inflamed and painful.
Symptoms
Most children with Sever's complain of pain in the heel that occurs during or after activity (typically running or jumping) and is usually relieved by rest. The pain may be worse when wearing cleats. Sixty percent of children's with Sever's report experiencing pain in both heels.
Diagnosis
All medical diagnosis should be made by taking a full history, examining the patient then performing investigations. The problem usually occurs in boys who are going through or have just gone through a growth spurt; one or both heels may be affected. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. There may be swelling over the back of the heel and this area is painful if touched or knocked. On examination the patient often has flat feet, very tight legs muscles especially the gastrocnemius.
Non Surgical Treatment
Fortunately Severs? disease can be treated and prevented through a number of different techniques that have all proven highly effective. The heel will repair itself even without active treatment provided that the suffering foot is given a chance to heal. Typically Severs? disease will take 2-8 weeks, although in many cases it can take longer as the continuous growing of the bone can exacerbate the condition. Podiatrists have an important role in preventing Severs? disease in young athletes, and in treating the condition when it develops so children can get back on their feet as quickly as possible. Generally treatment involves stretching muscles running down to the heel to relieve tension and pain, these include the hamstrings and calf muscles, and these stretching exercises will need to be performed at least 2 or 3 times a day. RICE is a classic method of speeding up the recovery of self-healing injuries like Severs? disease. This involves Rest, the application of Ice to the injury, Compression, and finally Elevation to encourage repaid. These measures can be advised by a trained podiatrist, but it is then up to a child to carry on with regular RICE.
Prevention
After the painful symptoms of Sever's disease have gone away, it is important to continue stretching the heel, particularly before a vigorous exercise, and wearing good supportive shoes fitted with children's arch supports. This will prevent heel pain recurrence until the child's heel is fully developed and less prone to injury.
Sever's disease involves a lesion to the heel that appears mostly as a result of excessively twisting the ankle. The injury is particularly prevalent in children over 10 and other younger athletes because the heel bone, muscles and tendons are still developing - the bone faster than the muscles - and the condition strikes a growing part of the bone called the calcaneal apophysis. In older people an injury of this sort generally results in a stress fracture.
Causes
There are several theories as to the cause of this condition. These range from a tight Achilles tendon, to micro stress fractures of the calcaneal apopyhsis. The prevailing theory suggests that the condition occurs when the child's growth plate is at its weakest. Combined with increased athletic activity, improper shoe gear and trauma the heel becomes inflamed and painful.
Symptoms
Most children with Sever's complain of pain in the heel that occurs during or after activity (typically running or jumping) and is usually relieved by rest. The pain may be worse when wearing cleats. Sixty percent of children's with Sever's report experiencing pain in both heels.
Diagnosis
All medical diagnosis should be made by taking a full history, examining the patient then performing investigations. The problem usually occurs in boys who are going through or have just gone through a growth spurt; one or both heels may be affected. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. There may be swelling over the back of the heel and this area is painful if touched or knocked. On examination the patient often has flat feet, very tight legs muscles especially the gastrocnemius.
Non Surgical Treatment
Fortunately Severs? disease can be treated and prevented through a number of different techniques that have all proven highly effective. The heel will repair itself even without active treatment provided that the suffering foot is given a chance to heal. Typically Severs? disease will take 2-8 weeks, although in many cases it can take longer as the continuous growing of the bone can exacerbate the condition. Podiatrists have an important role in preventing Severs? disease in young athletes, and in treating the condition when it develops so children can get back on their feet as quickly as possible. Generally treatment involves stretching muscles running down to the heel to relieve tension and pain, these include the hamstrings and calf muscles, and these stretching exercises will need to be performed at least 2 or 3 times a day. RICE is a classic method of speeding up the recovery of self-healing injuries like Severs? disease. This involves Rest, the application of Ice to the injury, Compression, and finally Elevation to encourage repaid. These measures can be advised by a trained podiatrist, but it is then up to a child to carry on with regular RICE.
Prevention
After the painful symptoms of Sever's disease have gone away, it is important to continue stretching the heel, particularly before a vigorous exercise, and wearing good supportive shoes fitted with children's arch supports. This will prevent heel pain recurrence until the child's heel is fully developed and less prone to injury.
Post Achilles Tendon Rupture Exercises
Overview
 Rupture of Achilles tendon is the most common among those taking place in the lower extremities, being twice as common in men than in women between 30-50 years old and usually caused while doing sport. There are some risk factors such as age or chronic treatments based on corticosteroids or antibiotics when belonging to Quinolones group. Spontaneous bilateral rupture of the Achilles tendon is much more infrequent, being almost exceptional in young and healthy patients without known pathological conditions.
Rupture of Achilles tendon is the most common among those taking place in the lower extremities, being twice as common in men than in women between 30-50 years old and usually caused while doing sport. There are some risk factors such as age or chronic treatments based on corticosteroids or antibiotics when belonging to Quinolones group. Spontaneous bilateral rupture of the Achilles tendon is much more infrequent, being almost exceptional in young and healthy patients without known pathological conditions.
Causes
Repeated stress from a variety of causes is often the cause of Achilles tendon injury. The stress may occur from any of the following. Excessive activity or overuse. Flat feet. Poorly fitting or inadequate shoes. Inadequate warm-up or proper conditioning. Jogging or running on hard surfaces. Older recreational athlete. Previous Achilles tendon injury (tendonitis/rupture). Repeated steroid injections. Sudden changes in intensity of exercise. Use of fluoroquinolone antibiotics (especially in children). Trauma to the ankle. Tense calf muscles prior to exercise. Weak calf muscles.
Symptoms
Symptoms usually come on gradually. Depending on the severity of the injury, they can include Achilles pain, which increases with specific activity, with local tenderness to touch. A sensation that the tendon is grating or cracking when moved. Swelling, heat or redness around the area. The affected tendon area may appear thicker in comparison to the unaffected side. There may be weakness when trying to push up on to the toes. The tendon can feel very stiff first thing in the morning (care should be taken when getting out of bed and when making the first few steps around the house). A distinct gap in the line of the tendon (partial tear).
Diagnosis
An Achilles' tendon injury can be diagnosed by applying the Thompson Test (or Calf Squeeze Test) this is where the person who has suffered the injury lies on their front with their legs bent. Whoever is performing the test, usually a doctor, will then squeeze the calf muscle. If the tendon has not ruptured then the foot should point briefly away from the leg.
Non Surgical Treatment
Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome. 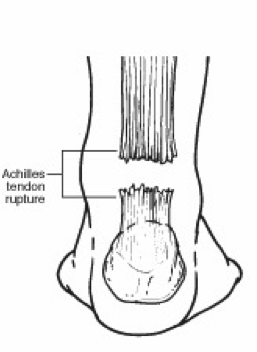
Surgical Treatment
Surgery is recommended to those who are young to middle-aged and active. The ruptured tendon is sewn together during surgery. This is an outpatient procedure. Afterward the leg is put into a splint cast or walking boot. Physical therapy will be recommended. In about 4 to 6 months, healing is nearly complete. However, it can take up to a year to return to sports fully.
Leg Length Discrepancy Special Test
Overview
Many children have one leg that is marginally longer than the other. In most cases, the difference is present at birth but may be too slight to be detected. More significant leg length differences (more than 2 cm) often become obvious as your child grows and begins to crawl and walk. We don?t always know what causes these discrepancies. A significant discrepancy can lead to more serious problems including arthritis and difficulty walking. However, with appropriate treatment, most children with this condition can participate in regular activities. Treatment options include heel lifts and, in more severe cases, surgery to either lengthen or shorten a leg.
Causes
Leg discrepancy can develop from a medical issue in any portion of the femur or tibia. One leg may lengthen, but leg shortening is much more common. Factors that can cause leg length discrepancy include inherited growth deficiencies. Infections. A bone infection can cause delayed growth in the affected limb. Injury. If your child breaks a leg, it may be shorter once it heals. This is most likely to happen if the fracture or break was complicated, an open fracture, or an injury that affected the growth plate near the end of the bone. Alternatively, a break can cause bones to grow faster after healing, making a leg longer. Tumors. Legg-Calve-Perthes disease. This is a condition that affects the ball (femoral head) of the hip joint. The femoral head may be friable and damage easily, sometimes leading to shortening of the thigh bone. Hemihypertrophy. In children with this condition, one side of the body grows more quickly than the other. Vascular malformations. These are abnormal clusters of veins and arteries that can form close to the bone and stimulate growth. Juvenile arthritis. Inflammation from arthritis can stimulate growth in the affected leg and cause discrepancy.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.

Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Many children have one leg that is marginally longer than the other. In most cases, the difference is present at birth but may be too slight to be detected. More significant leg length differences (more than 2 cm) often become obvious as your child grows and begins to crawl and walk. We don?t always know what causes these discrepancies. A significant discrepancy can lead to more serious problems including arthritis and difficulty walking. However, with appropriate treatment, most children with this condition can participate in regular activities. Treatment options include heel lifts and, in more severe cases, surgery to either lengthen or shorten a leg.
Causes
Leg discrepancy can develop from a medical issue in any portion of the femur or tibia. One leg may lengthen, but leg shortening is much more common. Factors that can cause leg length discrepancy include inherited growth deficiencies. Infections. A bone infection can cause delayed growth in the affected limb. Injury. If your child breaks a leg, it may be shorter once it heals. This is most likely to happen if the fracture or break was complicated, an open fracture, or an injury that affected the growth plate near the end of the bone. Alternatively, a break can cause bones to grow faster after healing, making a leg longer. Tumors. Legg-Calve-Perthes disease. This is a condition that affects the ball (femoral head) of the hip joint. The femoral head may be friable and damage easily, sometimes leading to shortening of the thigh bone. Hemihypertrophy. In children with this condition, one side of the body grows more quickly than the other. Vascular malformations. These are abnormal clusters of veins and arteries that can form close to the bone and stimulate growth. Juvenile arthritis. Inflammation from arthritis can stimulate growth in the affected leg and cause discrepancy.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.
Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
What Causes Posterior Tibial Tendon Dysfunction ?
Overview
This condition is a progressive collapse of the tendons and ligaments that hold up the foot?s arch. This condition most commonly affects women. It typically occurs in only one foot, but in some cases, both feet are afflicted. 
Causes
There are a number of theories as to why the tendon becomes inflamed and stops working. It may be related to the poor blood supply within the tendon. Increasing age, inflammatory arthritis, diabetes and obesity have been found to be causes.
Symptoms
Symptoms are minor and may go unnoticed, Pain dominates, rather than deformity. Minor swelling may be visible along the course of the tendon. Pain and swelling along the course of the tendon. Visible decrease in arch height. Aduction of the forefoot on rearfoot. Subluxed tali and navicular joints. Deformation at this point is still flexible. Considerable deformity and weakness. Significant pain. Arthritic changes in the tarsal joints. Deformation at this point is rigid.
Diagnosis
Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot.
Non surgical Treatment
Initial treatment for most patients consists of rest and anti-inflammatory medications. This will help reduce the swelling and pain associated with the condition. The long term treatment for the problem usually involves custom made orthotics and supportive shoe gear to prevent further breakdown of the foot. ESWT(extracorporeal shock wave therapy) is a novel treatment which uses sound wave technology to stimulate blood flow to the tendon to accelerate the healing process. This can help lead to a more rapid return to normal activities for most patients. If treatment is initiated early in the process, most patients can experience a return to normal activities without the need for surgery. 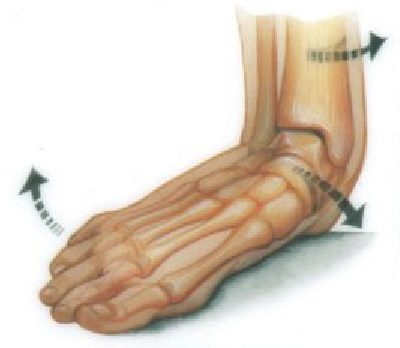
Surgical Treatment
A new type of surgery has been developed in which surgeons can re-construct the flat foot deformity and also the deltoid ligament using a tendon called the peroneus longus. A person is able to function fully without use of the peroneus longus but they can also be taken from deceased donors if needed. The new surgery was performed on four men and one woman. An improved alignment of the ankle was still evident nine years later, and all had good mobility 8 to 10 years after the surgery. None had developed arthritis.